
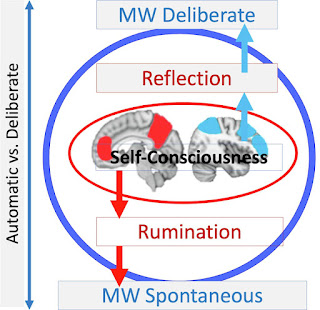
“The self is the psychological counterpart of the default mode functionality of the brain.” (Scalabrini et al., 2021).
The self that studies how the “Self” is represented and constructed by the brain is apex meta-neuroscience.1 We can say that the self is a manifestation (or an illusory by-product) of activity in the default mode network (medial prefrontal cortex, posterior cingulate cortex/precuneus and angular gyrus), but what does this really mean? How do we relate specific neural states to aspects of a changing self? In a field that increasingly focuses on the remote control of genetically defined microcirculations, it seems assumed and hopelessly overambitious to discover subjective internal phenomena.
But of course, the inherent challenge of studying complex subjective experiences hasn’t stopped researchers from trying. An active area of research involves characterizing the neural correlates of internal responses to traumatic events. This is of great clinical relevance, because long-term persistent fear, hypervigilance, negative affect and intrusive memories after trauma can be disabling (post-traumatic stress disorder, PTSD). Changes in one’s sense of self (dissociation) can also occur in PTSD, and is the focus of the rest of this post. Dissociative symptoms may include:
-
Depersonalization: Persistent or recurrent experiences of feeling detached from, and as if an outside observer of, one’s mental processes or body (eg, feeling as if one were in a dream; feeling unreality in self or body or that time is moving slowly).
-
Derealization:
Persistent or recurring experiences of the unreality of the environment (eg the world around the individual is experienced as unreal, dreamlike, distant or distorted).
In states of depersonalization/derealization (which can occur independently of PTSD), one feels disconnected from the self and/or external reality. Dissociative symptoms are considered a maladaptive (but protective) response to stress and trauma. The standard method for eliciting dissociative symptoms during fMRI scanning is script-driven imagery (SDI), a highly unpleasant manipulation. Before the experiment, the participant tells a narrative about the traumatic event, which is then read back to them in the scanner. The presence of acute dissociative symptoms is determined by questionnaires and interviews before, during and after the scan.
Early studies reported increased activity in prefrontal (and other) cortical regions in the SDI condition compared to baseline (Lanius et al., 2002) or a neutral script condition (Hopper et al., 2007), which was related to the severity of dissociative symptoms. This fits in a theoretical perspective where higher cortical regions moderate limbic (and emotional) responses to the trauma induction. It should be mentioned that dissociative responses to SDI are generally less common than vivid re-experiencing of the trauma (30% vs. 70% in Lanius et al., 2002). Disadvantages of these studies include small sample sizes and inconsistencies in the fMRI results.
Mertens and colleagues (2022) set out to replicate these findings in a larger, more homogeneous population of 51 female survivors of childhood abuse. The study included additional questionnaires and separation of the SDI condition into “script listening” and “focused recall” phases (previous studies included only the latter). The experimental design included three series of neutral script (30 sec each with listening/image processing and focused recall of the event) and three series of trauma script, which were effective in increasing self-reported ratings of dissociative symptoms, e.g.Did what you experienced seem unreal to you, as if you were in a dream or watching a movie or play?” and “Did you feel like you were a bystander watching what happened to you, like an observer or outsider?” (rated on a scale from 0-6).
– click on the image for a larger view –
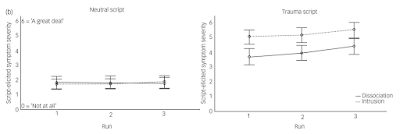
The fMRI results indicated that a broad range of the left cerebellum, occipital cortex, and supramarginal gyrus (parietal lobe) were more active in the trauma script than the neutral condition, and this was specific to the script listening phase (no differences were observed during the focused recall phase). The same pattern was seen in the amygdala in a region of interest analysis. Importantly, there was no correlation between any of the clusters and any dissociation measure (amygdala and insula shown below).2

Fig. 2 (Mertens et al., 2022). Script-triggered signal activation clusters and corresponding brain-behavior correlates (N = 51).
The authors tried a number of different analytical techniques to find a link between activation clusters and dissociative symptoms, but they failed. In their conclusions, they mentioned the importance of the replication crisis in neuroimaging and noted that “the current (null) findings highlight the difficulty of extracting reliable neurobiological biomarkers for complex subjective experiences such as dissociation.” Identifying who we are and what we experience via spatial and temporal patterns of brain activity are problems that have no immediate solution.
Footnotes
1 Self = a self-aware entity with fully realized consciousness (whatever this means)
2 Here, the number of self-report and clinician-rated measures was impressive, e.g. The Dissociative Experiences scale (trait dissociation), Cambridge Depersonalization Scale, Clinician Administered Dissociative States Scale, Responses to Script-Driven Imagery, etc.
Further reading
Feeling Mighty Unreal: Derealization in Kleine-Levin Syndrome
A detached sense of self-esteem associated with altered neural responses to mirror touch
The role of the vestibular system in the construction of the self
Derealization / dying
‘I Do Not Exist’ – Pathological loss of self after a Buddhist retreat
The stranger in the mirror
Writing-induced joint condition
References
Hopper JW, Frewen PA, van der Kolk BA, Lanius RA. (2007). Neural correlates of reexperiencing, avoidance, and dissociation in PTSD: Symptom dimensions and emotion dysregulation in response to script-driven trauma imagery. Journal of Traumatic Stress 20(5):713-25.
Lanius RA, Williamson PC, Boksman K, Densmore M, Gupta M, Neufeld RW, Gati JS, Menon RS. (2002). Brain activation during script-driven imagery induced dissociative responses in PTSD: a functional magnetic resonance imaging study. Biological psychiatry 52(4):305-11.
Lebois LA, Harnett NG, van Rooij SJ, Ely TD, Jovanovic T, Bruce SE, House SL, Ravichandran C, Dumornay NM, Finegold KE, Hill SB et al. (2022). Persistence of dissociation and its neural correlates predicting outcome after trauma exposure. American Journal of Psychiatry June 22.
Mertens YL, Manthey A, Sierk A, Walter H, Daniels JK. (2022). Neural correlates of acute posttraumatic dissociation: a functional neuroimaging script-driven imaging study. BJPsych Open 8(4).
Northoff G, Scalabrini A. (2021). “Project for a Spatiotemporal Neuroscience” – Brain and psyche share their topography and dynamics. Frontiers in psychology 2021:4500.
Scalabrini A, Schimmenti A, De Amicis M, Porcelli P, Benedetti F, Mucci C, Northoff G. (2022). The self and its inner thought: In search of a psychological baseline. Awareness and cognition 97:103244.
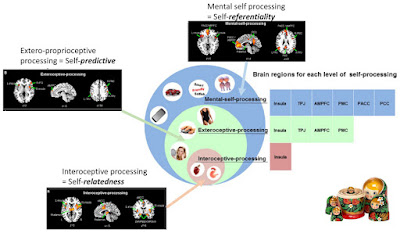
Fig. 4 (Northoff & Scalabrini, 2021). Nested hierarchy of the self in the brain.





