
March 18, 2026
3 my read
 Add us on GoogleAdd SciAm
Add us on GoogleAdd SciAm
COVID probably killed 150,000 more people in its first two years than official US tolls show
We have seriously underestimated the number of COVID deaths, say researchers

White flags are displayed in front of the Washington Monument in a 2021 commemoration of those killed by COVID.
Douglas Rissing/Getty Images
COVID may have killed significantly more people in the United States during the first two years of the pandemic than official records indicate, with as many as one overlooked death for every five recorded. That brings the total to nearly one million deaths in 2020 and 2021 alone.
This calculation comes from research published today in The progress of science which seeks to understand how many COVID deaths fell through the cracks of official reporting systems. The full cases show that the burden of the pandemic in the United States fell most heavily on marginalized people.
“These vulnerable groups just take a higher risk at each step, and the accumulation of all of this is this disparity in COVID mortality at the end,” says Mathew Kiang, an epidemiologist at Stanford University and co-author of the study.
On supporting science journalism
If you like this article, please consider supporting our award-winning journalism by subscribes. By purchasing a subscription, you help secure the future of impactful stories about the discoveries and ideas that shape our world today.
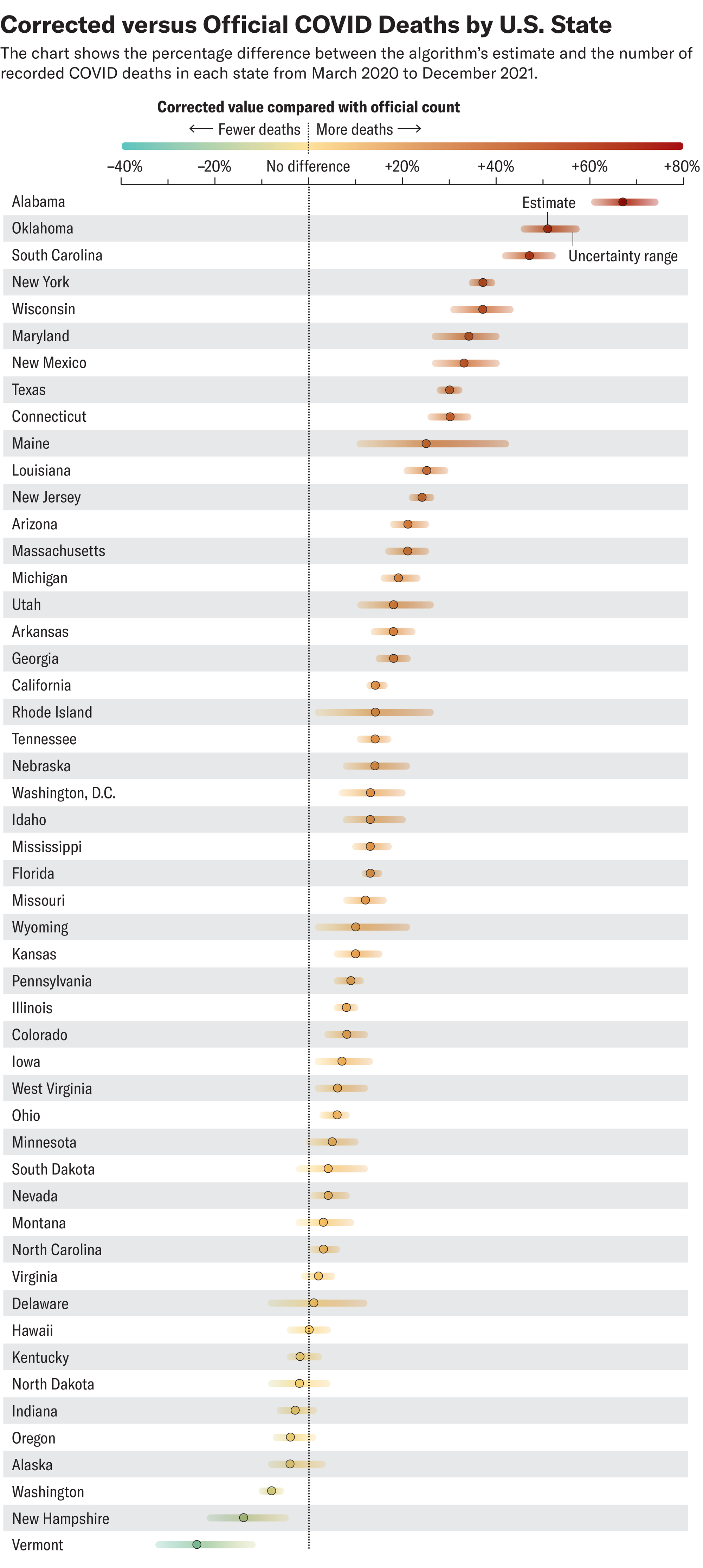
In the new research, Kiang and colleagues analyzed official records published by the Centers for Disease Control and Prevention for deaths that occurred from March 2020 to December 2021 for adults aged 25 and older — about 5.7 million records in total. First, they fed a machine learning algorithm with records of deaths in hospitals, which at the time tested most patients for COVID. They trained the algorithm to recognize hospital deaths where COVID was formally identified as an underlying cause. They then used the algorithm to flag potential unknown COVID deaths by identifying records that looked like hospitalized COVID deaths but occurred in other settings where testing was less likely.
All told, the algorithm identified between about 150,000 and 160,000 potential unknown COVID deaths on top of the 840,251 that were officially reported. These figures suggest that for every five recognized COVID deaths, one additional death went unnoticed. That ratio is on par with other analyzes that have simply compared the total observed number of deaths with the number of total deaths expected based on historical data, said Daniel Weinberger, an epidemiologist at the Yale School of Public Health, but the new method is both more sophisticated and more granular.
Kiang says it is not surprising that deaths from COVID were missed. “Death reporting in the United States is a fragmented, under-resourced infrastructure,” he says. “During the pandemic, it was very strained. We had more deaths than we had ever had” in modern history.
But what stood out to him were the patterns behind the unknown likely COVID deaths: they were most likely to have occurred among Hispanics, at home, among the less educated and among people with lower incomes. When analyzed by state, Alabama, Oklahoma and South Carolina had the highest rates of such deaths.
These patterns tell an important story about how COVID played out in the United States and its fragmented healthcare systems. “This underreporting that we found was not accidental,” says Kiang. “Quite systematically, what we found was that communities in areas most affected by the pandemic were also those with the most unknown COVID-19 mortality.” By analyzing the dramatic case of the early years of the COVID pandemic, researchers can better understand how the same factors that made people vulnerable to COVID affect more routine health conditions, Kiang says.
During the pandemic, “systems in our society, including barriers to access to health care, kept desperately ill Americans from recognizing the need for care and getting to the hospital,” says Steven Woolf, a physician and social epidemiologist at Virginia Commonwealth University, who was not involved in the new research. He worries not only that these barriers remain, but that cuts to Medicaid and rising health insurance premiums could exacerbate them. “People on the margins continue to die at disproportionate rates because they don’t have access to care.”
It’s time to stand up for science
If you liked this article, I would like to ask for your support. Scientific American has served as an advocate for science and industry for 180 years, and right now may be the most critical moment in its two-century history.
I have been one Scientific American subscriber since I was 12 years old, and it helped shape the way I see the world. SciAm always educates and delights me, and inspires a sense of awe for our vast, beautiful universe. I hope it does for you too.
If you subscribe to Scientific Americanyou help ensure our coverage is centered on meaningful research and discovery; that we have the resources to report on the decisions that threaten laboratories across the United States; and that we support both budding and working scientists at a time when the value of science itself is too often not recognised.
In return, you receive important news, captivating podcasts, brilliant infographics, can’t-miss newsletters, must-see videos, challenging games, and the world of science’s best writing and reporting. You can even give someone a subscription.
There has never been a more important time for us to stand up and show why science is important. I hope you will support us in that mission.





